RefluxStop™ Results Published
When we founded RefluxUK the first thing we did was compose our RefluxUK Credo. We wrote down in black and white our vision, our focus and our principles. These define our guiding philosophy and provide a set of principles upon which we base all we do.

Written by Mr Nick Boyle
Among these principles we resolved to employ the best technology and innovations to improve outcomes. We also commit to share and publish our data to educate ourselves, patients and other clinicians but also to improve performance. We see this as a professional duty. So, introducing new technology and then publishing our results is part of the RefluxUK DNA. We’ve published our results on LINX including the largest UK study in which we reported 5-year outcomes in 200 patients as well as the relationship between SIBO and reflux symptoms; there’ll be more on this to follow!
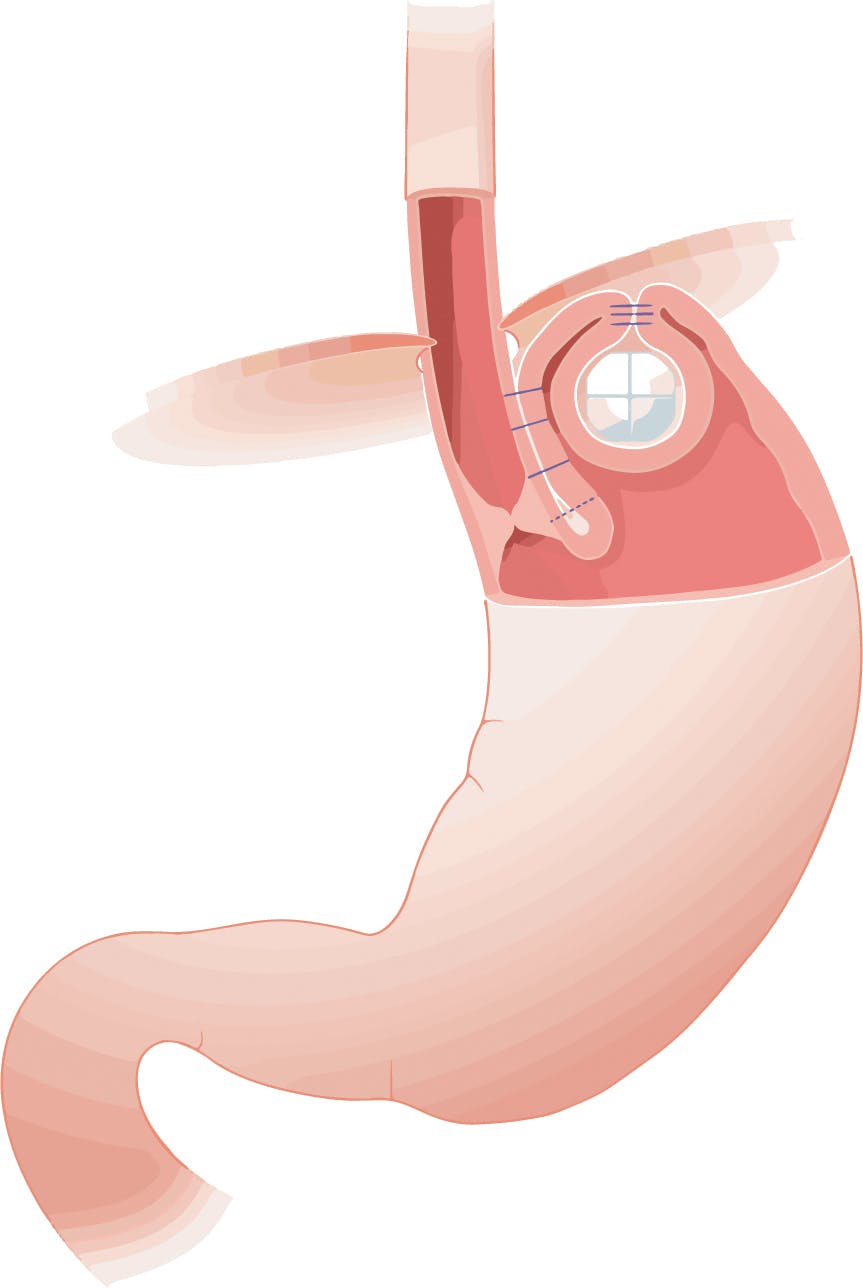
Consistent with this approach, in March 2022 we were the first in the UK to introduce RefluxStop. Since then we have performed over 50 procedures and have the largest experience in the UK. This “keyhole” operation involves implantation of a small silicon ball in the stomach having performed a “partial” fundoplication which helps to strengthen the lower oesophageal valve, in which the upper stomach (fundus) is stitched to the side of the oesophagus. It’s a technically complicated procedure and involves altering the normal anatomy significantly. However, the theoretical advantages of RefluxStop are that it offers a surgical option to patients who can’t undergo standard fundoplication, LINX or TIF because they have ineffective oesophageal motility. And early studies confirmed that “dysphagia”, the technical term for swallowing difficulties, is unusual after RefluxStop.
Ineffective oesophageal motility commonly affects patients with bad reflux. Often it is asymptomatic and demonstrated only when pre-operative high resolution manometry is performed. Some patients will experience swallowing difficulties. The concern is that when the strength of the muscular contractions that are responsible for normal swallowing fail, eating may be a problem after surgery when the valve has been strengthened with a procedure that effectively encircles the oesophagus.
So, we were delighted to join forces with Sebastian Schoppmann, Professor of Surgery at Vienna University, and his team to pool the results of 40 patients in who we’d undertaken RefluxStop and who all had ineffective motility. Professor Schoppmann is one of the leading and most respected reflux surgeons in Europe. To our knowledge, this is the first study looking at clinical outcomes in this group of patients. Our study has now been published in the prestigious scientific journal Nature Scientific Reports, the 5th most frequently cited journal in the world.
RefluxStop and Ineffective Motility, Nature Scientific Reports
The results are inevitably short term, at 3 months following RefluxStop surgery. However, quality of life scores improved significantly, measured by GERD HRQL. Both heartburn as well as regurgitation improved significantly. There was an 84% reduction of PPI usage. In 36 patients (90%) symptoms improved or resolved such that patients were satisfied with the outcome. Importantly, swallowing was a problem for just 1 patient. However, there were 2 adverse events in which the implant either slipped or eroded into the stomach; the former required further surgery and the second no intervention. We concluded that on the basis of these results RefluxStop is “safe and effective in the short term but that further studies and longer follow-up are necessary”.
So where does RefluxStop fit into the options? Our study has provided encouraging results but, in our view, it remains an experimental procedure. We lack medium, let alone long-term, data and simply don’t know how safe and effective the procedure is over time. It’s not a risk-free procedure although as experience grows we’ll hopefully learn how to minimise these. Most people wanting surgery are suitable for one of the established and proven options which we know are effective and which are supported by years of experience and published studies reporting outcomes in literally thousands of patients. And RefluxStop is an expensive procedure. However, in the context of ineffective motility, RefluxStop is an option that patients may wish to consider and this study provides evidence to support its use. For these patients it can offer relief from symptoms that would otherwise be unavailable. And so, RefluxUK offers RefluxStop on this basis.
A multi-national prospective and randomised study will start soon. Its results may provide the evidence that RefluxStop should be more widely offered. We await its results with keen interest. In the meantime, we will continue to innovate, introduce new techniques and publish the results.



